Answer
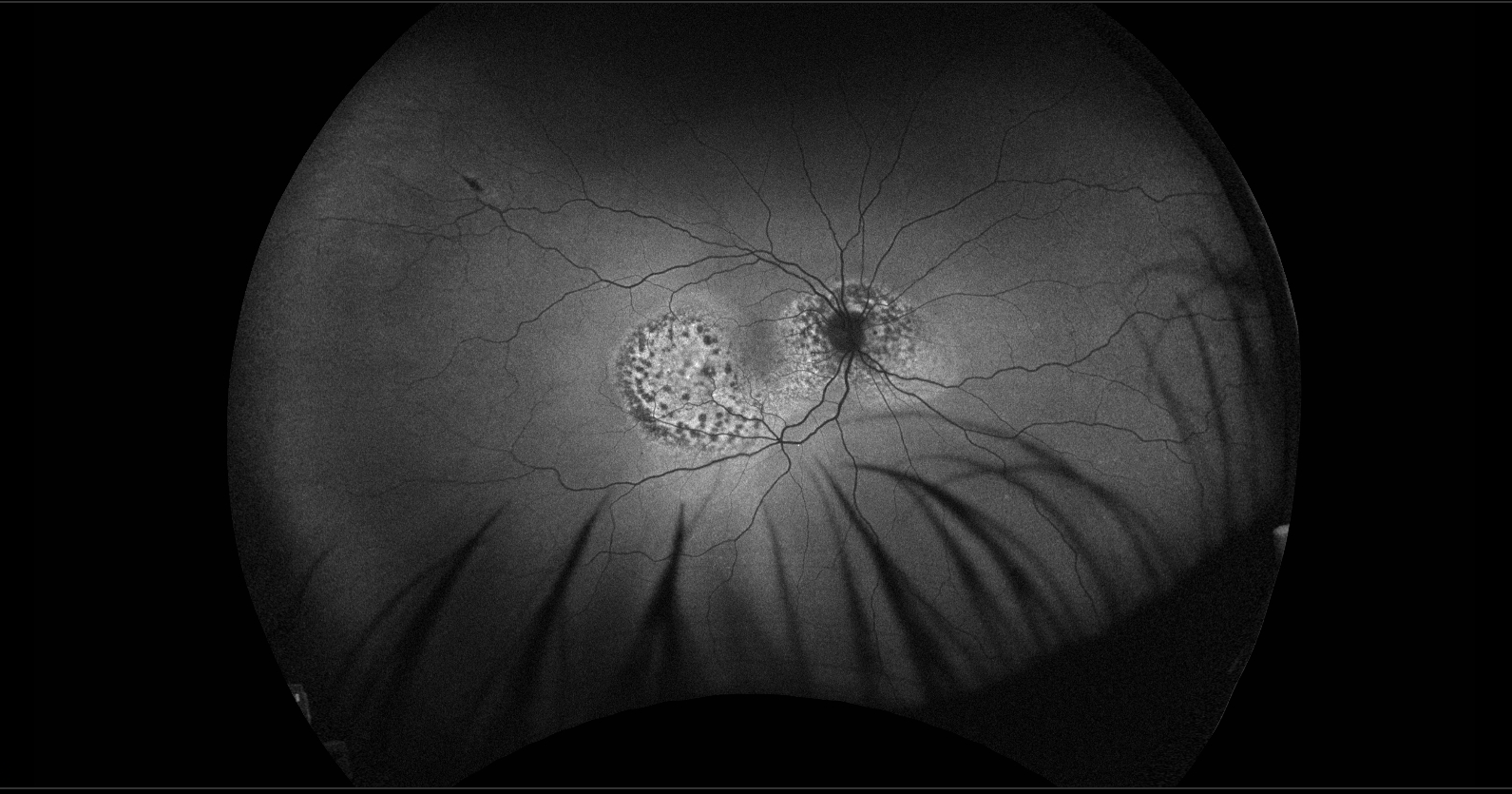
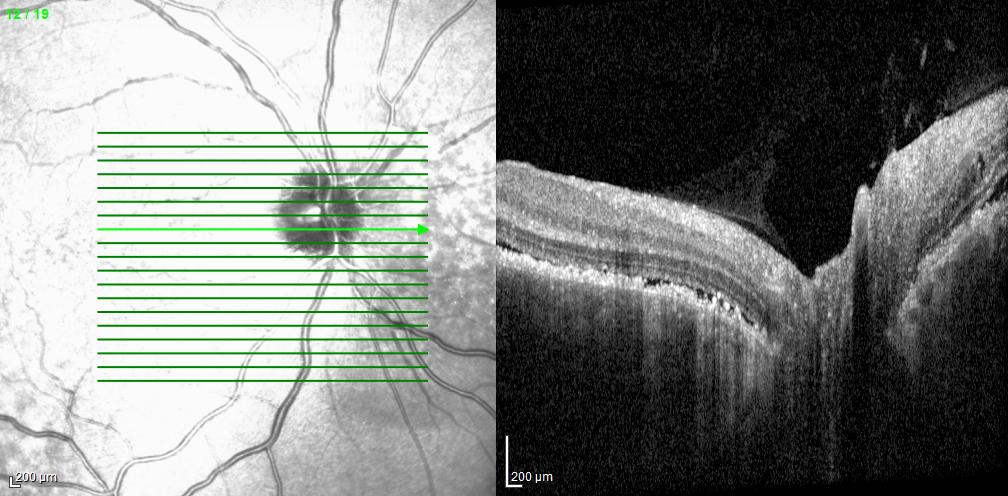
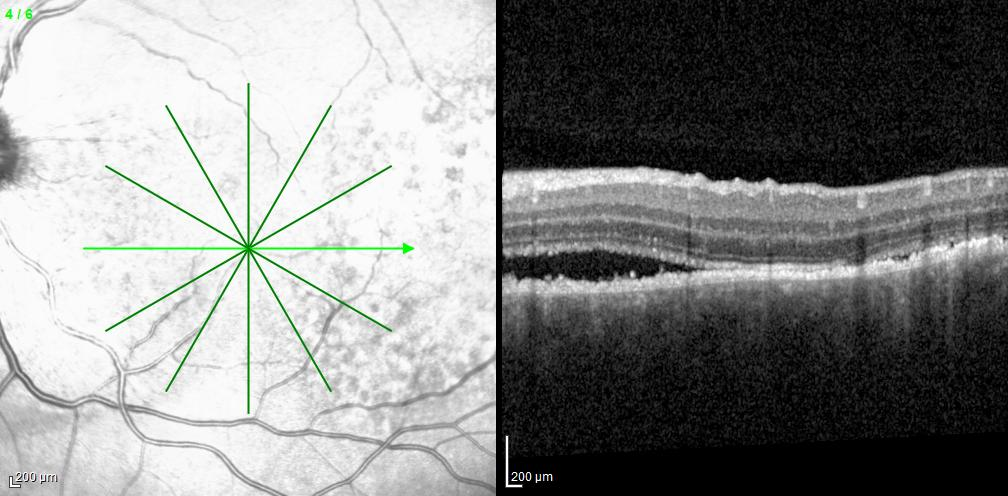
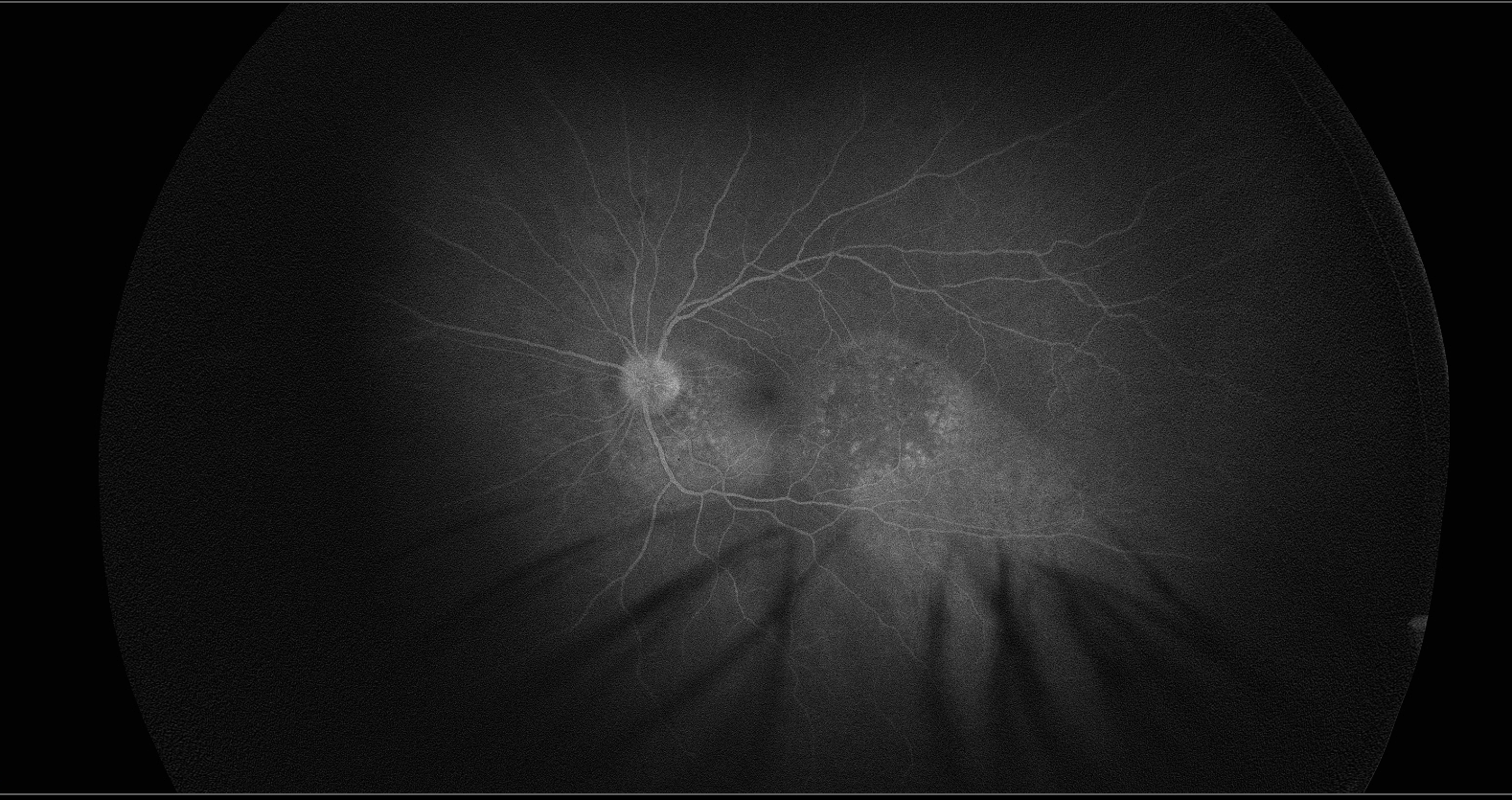
The autofluorescence studies demonstrated hypoautofluorescence corresponding to the small brown spots and hyperautofluorescence involving the remaining peripapillary and macular lesions in each eye. OCT of the right macula revealed irregular accumulation of subretinal hyperreflective material and serous subretinal fluid with tiny hyperreflective spots, disruption of the outer retinal layers and retinal pigment epithelium (RPE), and loss of the choroidal vasculature with partial sparing of the choriocapillaris. OCT around the right optic disc showed irregular thickening of the RPE with a thin overlying layer of serous subretinal fluid. OCT of the macula in the left eye demonstrated irregular thickening of the RPE, overlying serous subretinal fluid containing a few cells, and a similar loss of much of the choroidal vasculature. OCT of the left optic disc showed irregular thickening of the RPE corresponding to the areas of pigmentary change. Late fluorescein angiographic images revealed hyperfluorescence at the sites of the pigmented spots in each eye without leakage, likely due to staining of material at the level of the RPE. B-scan ultrasonography (not shown) was unremarkable.
This patient had bilateral diffuse uveal melanocytic proliferation (BDUMP), a rare paraneoplastic syndrome.1,2 BDUMP is characterized by uveal thickening with proliferation of benign melanocytes, clinically presenting as brown or faint orange spots or patches. The giraffe-like pattern seen in this case is atypical but has been reported previously.3 The pigmented lesions are generally larger than those observed in our patient. Approximately one-fifth of patients with BDUMP also develop pigmented and nonpigmented lesions on the iris and elsewhere in the body, including the skin and mucous membranes. In men, the associated primary malignancy is most commonly lung cancer or retroperitoneal carcinoma of uncertain origin, whereas in women it is usually carcinoma of the uterus or ovary. In most cases, BDUMP precedes the diagnosis of the underlying cancer.
BDUMP can result in severe localized retinal damage as well as extensive retinal detachment that is typically unresponsive to corticosteroids, antimetabolites, or radiation therapy. Plasmapheresis may be beneficial.4 Most patients die within two years of developing BDUMP.
1. Klemp K, Kiilgaard JF, Heegaard S, et al. Bilateral diffuse uveal melanocyticproliferation: Case report and literature review. Acta Ophthalmologia 2017; 95:439-45.
2. TongN, Wang L, Wang N, Zhou Z. Bilateral diffuse uveal melanocytic proliferationsecondary to rectal adenocarcinoma: A case report and literature review.Frontiers in Medicine 2021; 8:article 691686.
3. RahimyE, Soheilian M. Giraffe pattern of bilateral diffuse uveal melanocyticproliferation. Ophthalmology 2016; 123:483.
4. KatzMSJ, Leder HA, Choudhury T. Successful treatment of bilateral diffuse uvealmelanocytic proliferation with plasmapheresis. Journal of VitreoRetinalDiseases 2017; 1:420-3.